Respiratory Resource Center - LPT Medical
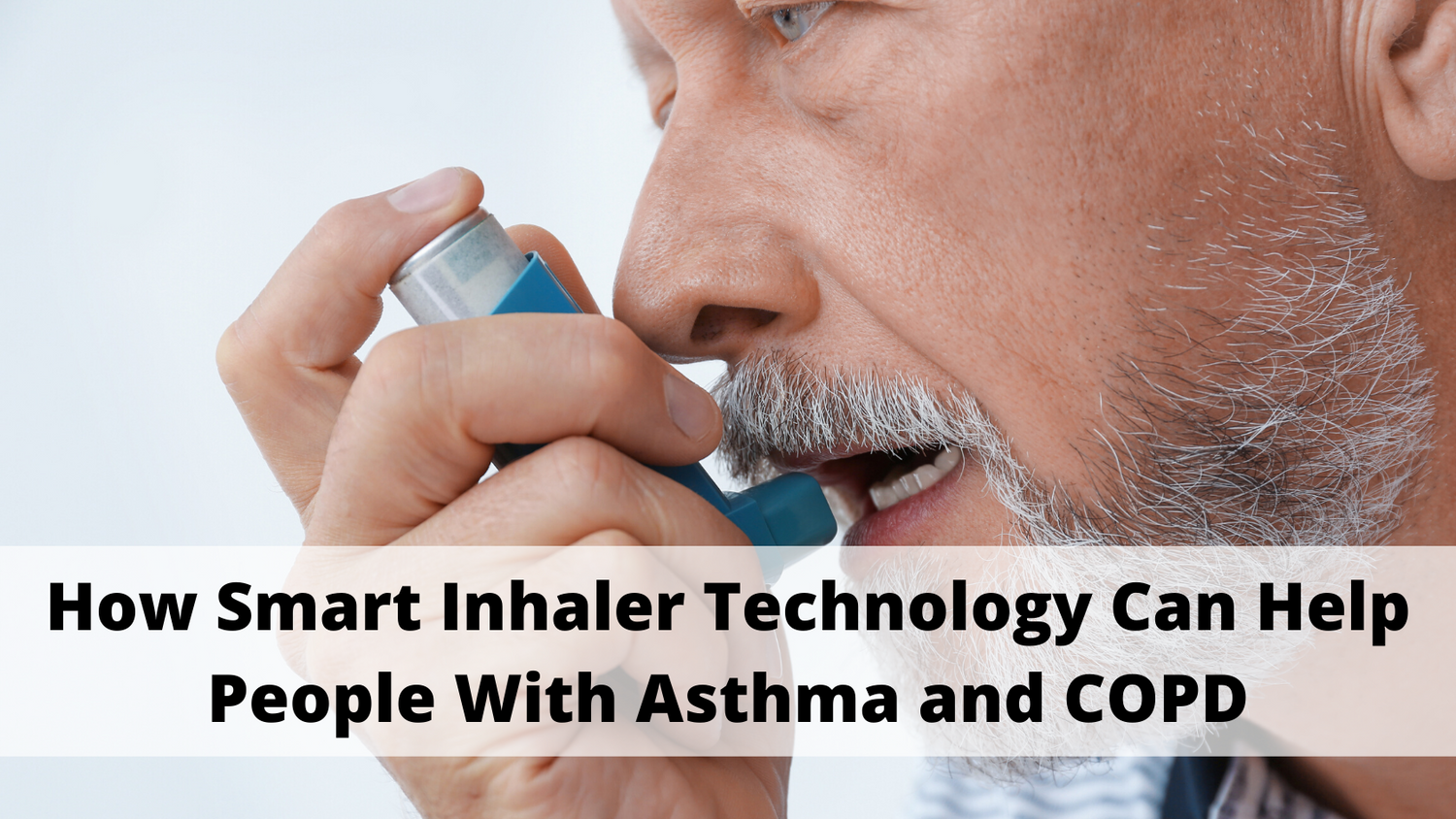
How Smart Inhaler Technology Can Help People With Asthma and COPD
Daily medications are a primary life-line for people with...
Read More
Standing Up for the Needs and Interests of People with COPD: The Vital Work of COPD Advocates
Despite the fact that COPD is the fourth...
Read More
How to Prepare for Medical Emergencies and Hospital Visits if You Have COPD
Consider this hypothetical scenario: you have a COPD...
Read More