
.png)
If you tuned into our blog earlier this month, you know that we discussed COPD as a “systemic disease.” In other words, it’s a disease that affects every part of the body, not just the lungs. This is an important distinction to make because it enables both patients and medical professionals to detect systemic manifestations earlier on and treat them more effectively. One of the systemic manifestations that we mentioned in this post is osteoporosis, a disease that affects the density of the bones.
{{cta('fa8abc2a-1e88-4fa3-82fd-1cb5b9ed43b2','justifycenter')}}
Osteoporosis is a common comorbidity of COPD, meaning the two conditions often exist side-by-side. Because of the nature of the two diseases, there are many complications that arise as a result of having them both. For example, both COPD and osteoporosis increase the patient’s risk of experiencing a fall as well as getting seriously injured from a fall. In this post, we’re going to take a closer look at the connection between COPD and osteoporosis, how they’re related, and how to cope with each. If you have any questions or concerns, be sure to leave them in the comment section below so that we can get back to you.
What is Osteoporosis?
Your bones are in a constant state of repair. Cells called osteoblasts synthesize bone material and assist in the mineralization of bone tissue. Simultaneously, cells called osteoclasts degrade old bone tissue and send calcium back into the blood. After a year, your body has regenerated about 10 percent of its bone tissue. The reason your body does this is that bone tissue does not last forever. It needs to be replaced regularly in order for your bones to be strong enough to support the weight of your body.
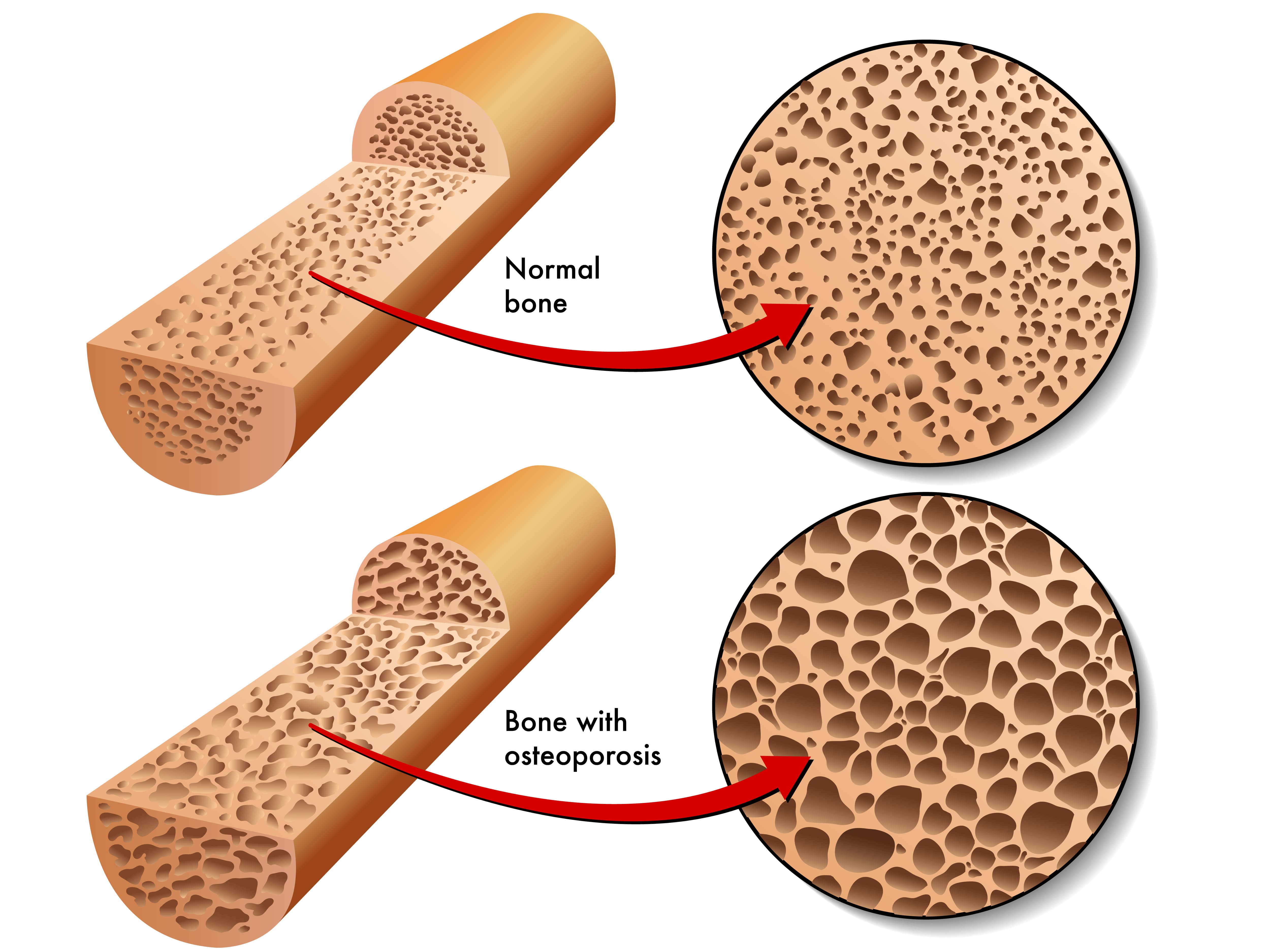
It’s natural for bone remodeling to occur more slowly the older we get. However, if the rate at which bone is produced is much slower than it’s being removed, or it’s being removed much quicker than it’s being replaced, this is known as osteoporosis, a disease that affects around 10 million Americans. Osteoporosis is more common in women over the age of 50, but anyone can get it at any age.
{{cta('b59df0c1-c4de-47a8-8e1c-0d33d4b414aa','justifycenter')}}
Osteoporosis usually develops very slowly and people are at a higher risk if they have a lower “peak bone mass.” Most people reach this point when they’re in their mid-twenties to thirties, so osteoporosis can sometimes (but not always) be predicted. Oftentimes, there are no warning signs of osteoporosis until the patient experiences a fracture. However, some people will experience joint pain, back pain, or a stooped posture. One instance where you may receive an early diagnosis of osteoporosis is if your doctor believes you are at high risk for this condition.

Bone fractures in the hip or spine are some of the most serious complications of osteoporosis because they impair the patient’s mobility. Falls are the most common cause of these types of injury but in severe cases, bones can fracture from simply bumping into something, bending over, or coughing. While there is no cure for osteoporosis there are many treatment options available that can help boost the rate of bone growth in your body, thus helping to prevent fractures and chronic pain.
How is Osteoporosis Diagnosed?
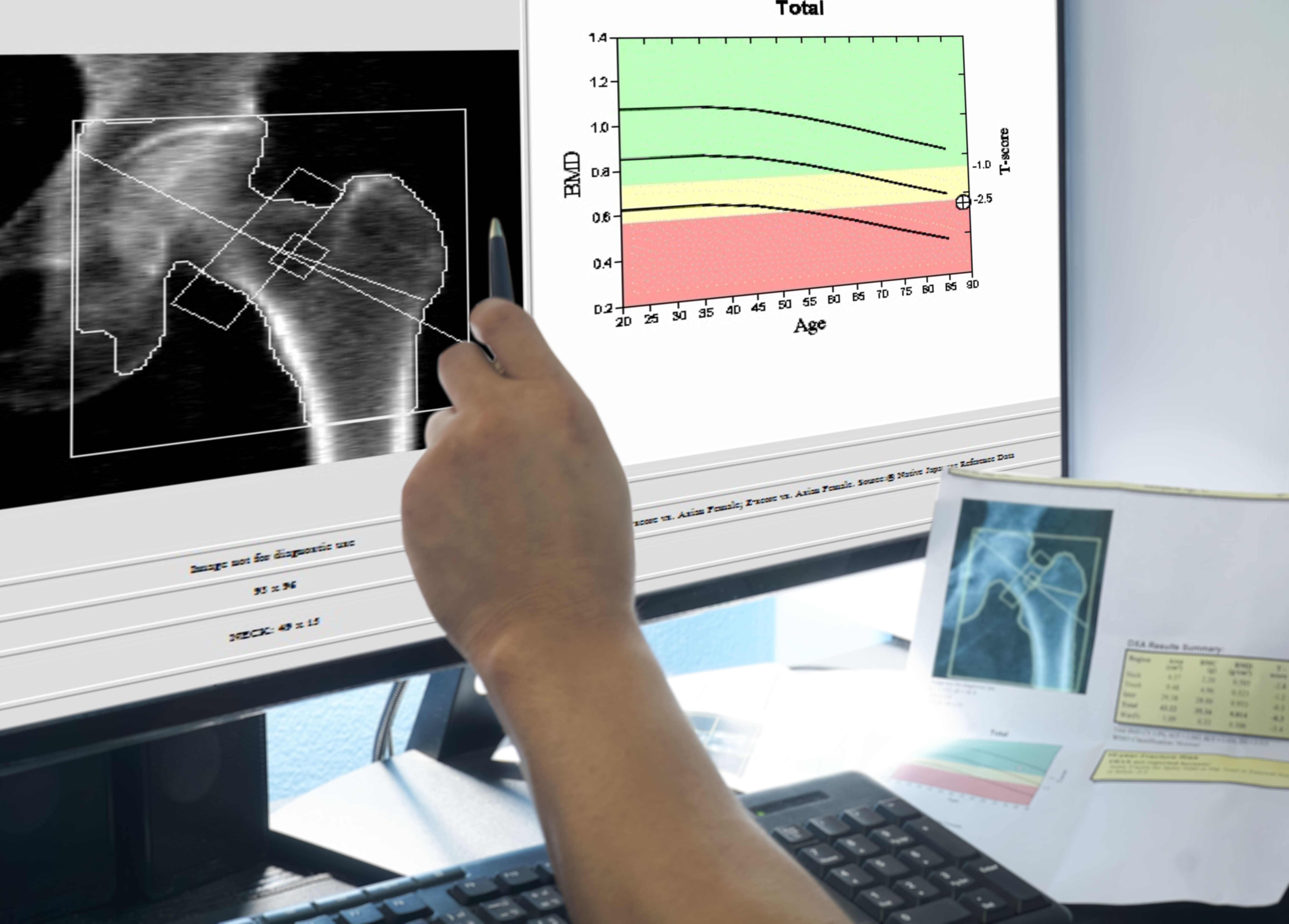
The main test used to diagnose osteoporosis is called a bone mineral density (BMD) test. It uses a type of low-energy X-ray called Dexa-Scan (dual-energy X-ray absorptiometry or DXA) to calculate the density of bone in the spine and hip. Your bone mineral density (BMD) is compared to the mean BMD for your age to determine if you have either osteoporosis or osteopenia. This is a condition that simply means you have low bone mineral density, it doesn’t necessarily mean that you will develop osteoporosis in the future or that you’re at risk of experiencing a fracture. If your BMD is less than one standard deviation below the mean, your bones are normal. Between -1 and -2.5 standard deviations is considered osteopenia and more than -2.5 is osteoporosis.
There are many other tests that can be performed to assist health professionals to determine if you have osteoporosis. Computerized tomography (CT) scans, X-rays, ultrasounds, and body composition analysis which shows the percentage of body weight due to bone, fat, muscle, and water. There are also many blood tests that can assist in diagnosing osteoporosis including blood calcium tests, vitamin D tests, thyroid tests, and testosterone tests. Be sure to ask your doctor if you’re not sure which test you need to take.
What’s the Link Between COPD and Osteoporosis?
At first glance, you might notice a lot of similarities between COPD and osteoporosis. Both conditions are more common in older adults, more common in women, and they can’t be cured. However, they’re both highly treatable. In other words, you’re at a higher risk of contracting COPD and osteoporosis based on your age and gender alone. But when you take a closer look, you’ll notice that there are many common side-effects of COPD that put you at a higher risk of osteoporosis in old age.

According to a study published by the National Health and Nutrition Examination Survey (NHANES) which included 14,828 subjects over the age of 45, there was an 8.5% prevalence of osteoporosis in non-COPD patients, but there was a prevalence of 16.9% in COPD patients. Let’s take a look at some of the side effects of COPD that may lead to osteoporosis.
A History of Smoking
Smoking is the most common preventable cause of morbidity and mortality worldwide. Smoking has countless systemic effects ranging from lung cancer to heart disease. Studies have also shown for decades that tobacco use has extremely adverse effects on bone health, not least of which is decreased bone density. According to UCI Health, there are several reasons why smoking is so bad for bone health. Firstly, it reduces the flow of blood to your bones by causing your blood vessels to constrict. This means your bones are being deprived of vital resources including osteoblasts, the bone-producing cells. Smoking has also been shown to hamper the resorption of calcium meaning it can’t be replaced in the bones.

There isn’t much to say about smoking and COPD that hasn’t already been said. According to the American Lung Association, about 85 to 90 percent of COPD cases are caused by cigarette smoking. What’s more, about 38 percent of people with COPD continue to smoke after receiving a diagnosis. It goes without saying that, if you’re a current smoker, the sooner you quit, the better. The respiratory effects of smoking are bad enough on their own, but when they’re combined with chronic pain and an increased risk of fractures, these issues are exacerbated.
Diet
Your body needs a large variety of vitamins and minerals in order to maintain every bodily function from digestion to blood flow. But when you develop a chronic condition, you often need to adjust your diet to accommodate for certain deficiencies that you may develop. In COPD and many other respiratory diseases, vitamin D deficiency is very common. Vitamin D is essential for everyone because it plays a vital role in helping your body absorb calcium which is the main support structure for your bones. Without it, your bones will become weak and brittle.

One of the main reasons respiratory patients are vitamin D deficient is that they oftentimes aren’t exposed to as much sunlight as their healthy counterparts. Sunlight is the most important natural source of vitamin D, but many COPD patients are immobilized by symptoms like fatigue, breathlessness, and chronic pain. One way to combat this is to simply sit by a window where you’re receiving direct sunlight. If you live in an area that doesn’t receive sunlight for prolonged parts of the year, you can supplement your diet with vitamin D-rich foods like oily fish, red meat, or egg yolks.
Body Mass Index (BMI)
Body mass index is derived from your body weight and height. Anything between a BMI of 18.5 and 24.9 is normal, but if you dip below this or go above it, it may be cause for concern. While the United States suffers from an obesity epidemic, COPD patients often suffer from the opposite problem — being underweight. According to the Lung Institute, COPD patients burn an average of 10 times as many calories while breathing as their healthy counterparts do. This is why many doctors recommend that COPD patients increase their caloric intake after being diagnosed. According to Healthline, about 25 to 40 percent of people with COPD have low body weight.

Having a BMI under 21 is also a risk factor for low bone mineral density (BMD) and osteoporosis. Studies have shown that BMI inversely correlates with BMD, so the lower your body weight is in comparison to your height, the more at risk you are for developing weak bones. As a COPD patient, the best thing you can do to prevent this is to ensure that you are eating enough and that you are following your doctor’s advice on what to eat. If you experience exhaustion from consuming large meals, try eating smaller meals all throughout the day in order to meet the calorie requirement that your doctor has set. This also helps your body out with digestion and prevents feelings of fatigue and bloating after eating.
Physical Activity
Exercise is one of the key components of an effective COPD treatment regime. Exercise keeps the lungs strong and healthy, reducing symptoms of breathlessness and chest pain. Strong muscles also use oxygen more effectively meaning you’ll be able to stay out of the house and stay active longer without taking a break. And while exercise can’t reverse COPD, it can improve your life expectancy and quality of life. Be sure to discuss with your doctor which exercise program will be best for you. Most health specialists recommend pulmonary rehabilitation which involves lung education, strength training, and endurance training.

According to Orthoinfor.aaos.org, exercise affects bones similar to how it affects muscle — it makes it stronger. Bone is living tissue and when stress is applied to it, it reacts by building more tissue. So, it goes without saying that, by exercising regularly, you can keep your bones in good condition and prevent osteoporosis. Unfortunately, due to the respiratory symptoms of COPD, many people are left feeling unmotivated or unable to exercise, and in turn, their bone health begins to suffer. You should aim to exercise at least 3 to 4 times per week and since hip and spinal fractures are most common in osteoporosis, be sure to get on your feet and work your whole body, not just your arms. Exercise also strengthens your stabilizer muscles, helping to improve balance and prevent falls.
COPD Medication
One final way that COPD affects your bones is through your medication. Your medication is a vital part of your treatment plan, but you have to be careful with it because, like any medication, it has both short- and long-term side effects. Most of the side effects should be listed on the container of the medication, but for more specific information, be sure to consult your doctor. The main COPD medication of concern when it comes to bone health is corticosteroids. These drugs are used by COPD patients to reduce inflammation which can prevent flare-ups and exacerbations. Corticosteroids are usually inhaled via an inhaler or nebulizer in order to reach the lungs more quickly.

The way that corticosteroids affect the bones is by altering the way the body uses vitamin D and calcium. Oftentimes, corticosteroids increase the rate at which bone breaks down and reduces its ability to absorb calcium. If corticosteroids are used heavily, this could lead to rapid bone deterioration, so it’s important to use them only as they’re prescribed. If you’re still concerned about bone loss even while taking the normal dosage, be sure to ask your doctor if there are any alternative medications that you can take without this side effect.
Conclusion
COPD is one of the most common chronic illnesses in the world. However, many people are unaware of the many systemic manifestations of this disease. About 36 to 60 percent of COPD patients have osteoporosis which is higher than the general population. The good news is that just a few lifestyle changes can significantly reduce your risk of experiencing low bone mineral density and osteoporosis. Immediate smoking cessation, a revised diet, regular physical activity, and careful use of your COPD medication are just a few of the most important.
If you’re a COPD patient who’s struggling to get on your feet and maintain an exercise routine, consider upgrading your obsolete oxygen device to a portable oxygen concentrator. POCs are much smaller and lighter than a standard oxygen tank meaning you won’t feel out of breath after a short walk. Portable oxygen concentrators like the Inogen One G5 and Caire FreeStyle Comfort have taken the oxygen industry by storm with a simple, easy-to-use interface, sleek design, and high oxygen output. If you’d like to learn more about these devices and all that they have to offer, don’t hesitate to reach out to our oxygen concentrator specialists here at LPT Medical.